Hydrocephalus can be defined broadly as a disturbance of formation, flow, or absorption of cerebrospinal fluid (CSF) that leads to an increase in volume occupied by this fluid in the CNS.[1] This condition also could be termed a hydrodynamic disorder of CSF. Acute hydrocephalus occurs over days, subacute hydrocephalus occurs over weeks, and chronic hydrocephalus occurs over months or years. Conditions such as cerebral atrophy and focal destructive lesions also lead to an abnormal increase of CSF in CNS. In these situations, loss of cerebral tissue leaves a vacant space that is filled passively with CSF. Such conditions are not the result of a hydrodynamic disorder and therefore are not classified as hydrocephalus. An older misnomer used to describe these conditions was hydrocephalus ex vacuo.
Normal pressure hydrocephalus (NPH) describes a condition that rarely occurs in patients younger than 60 years.[2] Enlarged ventricles and normal CSF pressure at lumbar puncture (LP) in the absence of papilledema led to the term NPH. However, intermittent intracranial hypertension has been noted during monitoring of patients in whom NPH is suspected, usually at night. The classic Hakim triad of symptoms includes gait apraxia, incontinence, and dementia. Headache is not a typical symptom in NPH.
Benign external hydrocephalus is a self-limiting absorption deficiency of infancy and early childhood with raised intracranial pressure (ICP) and enlarged subarachnoid spaces. The ventricles usually are not enlarged significantly, and resolution within 1 year is the rule.
Communicating hydrocephalus occurs when full communication occurs between the ventricles and subarachnoid space. It is caused by overproduction of CSF (rarely), defective absorption of CSF (most often), or venous drainage insufficiency (occasionally).
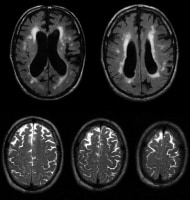 Communicating hydrocephalus with surrounding "atrophy" and increased
periventricular and deep white matter signal on fluid-attenuated inversion
recovery (FLAIR) sequences. Note that apical cuts (lower row) do not show
enlargement of the sulci, as is expected in generalized atrophy. Pathological
evaluation of this brain demonstrated hydrocephalus with no microvascular
pathology corresponding with the signal abnormality (which likely reflects
transependymal exudate) and normal brain weight (indicating that the sulci
enlargement was due to increased subarachnoid cerebrospinal fluid [CSF]
conveying a pseudoatrophic brain pattern).
Noncommunicating hydrocephalus occurs when CSF flow is obstructed within the
ventricular system or in its outlets to the arachnoid space, resulting in
impairment of the CSF from the ventricular to the subarachnoid space. The most
common form of noncommunicating hydrocephalus is obstructive and is caused by
intraventricular or extraventricular mass-occupying lesions that disrupt the
ventricular anatomy.[3]
Communicating hydrocephalus with surrounding "atrophy" and increased
periventricular and deep white matter signal on fluid-attenuated inversion
recovery (FLAIR) sequences. Note that apical cuts (lower row) do not show
enlargement of the sulci, as is expected in generalized atrophy. Pathological
evaluation of this brain demonstrated hydrocephalus with no microvascular
pathology corresponding with the signal abnormality (which likely reflects
transependymal exudate) and normal brain weight (indicating that the sulci
enlargement was due to increased subarachnoid cerebrospinal fluid [CSF]
conveying a pseudoatrophic brain pattern).
Noncommunicating hydrocephalus occurs when CSF flow is obstructed within the
ventricular system or in its outlets to the arachnoid space, resulting in
impairment of the CSF from the ventricular to the subarachnoid space. The most
common form of noncommunicating hydrocephalus is obstructive and is caused by
intraventricular or extraventricular mass-occupying lesions that disrupt the
ventricular anatomy.[3]  Noncommunicating obstructive hydrocephalus caused by obstruction of
the foramina of Luschka and Magendie. This MRI sagittal image demonstrates
dilatation of lateral ventricles with stretching of corpus callosum and
dilatation of the fourth ventricle.
Noncommunicating obstructive hydrocephalus caused by obstruction of
the foramina of Luschka and Magendie. This MRI sagittal image demonstrates
dilatation of lateral ventricles with stretching of corpus callosum and
dilatation of the fourth ventricle. 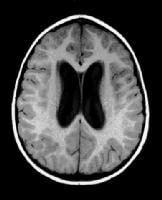 Noncommunicating obstructive hydrocephalus caused by obstruction of
foramina of Luschka and Magendie. This MRI axial image demonstrates dilatation
of the lateral ventricles.
Noncommunicating obstructive hydrocephalus caused by obstruction of
foramina of Luschka and Magendie. This MRI axial image demonstrates dilatation
of the lateral ventricles. 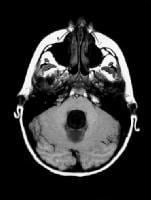 Noncommunicating obstructive hydrocephalus caused by obstruction of
foramina of Luschka and Magendie. This MRI axial image demonstrates fourth
ventricle dilatation.
Congenital hydrocephalus applies to the ventriculomegaly that develops in the
fetal and infancy periods, often associated with macrocephaly.[4] The most
common causes of congenital hydrocephalus are obstruction of the cerebral
aqueduct flow, Arnold-Chiari malformation or Dandy–Walker malformation.[5] these patients
may stabilize in later years due to compensatory mechanisms but may
decompensate, especially following minor head injuries. During these
decompensations, determining the extent to which any new neurological deficits
may be due to the new acute event, compared with hydrocephalus that may have
gone unnoticed for many years, is difficult.
Noncommunicating obstructive hydrocephalus caused by obstruction of
foramina of Luschka and Magendie. This MRI axial image demonstrates fourth
ventricle dilatation.
Congenital hydrocephalus applies to the ventriculomegaly that develops in the
fetal and infancy periods, often associated with macrocephaly.[4] The most
common causes of congenital hydrocephalus are obstruction of the cerebral
aqueduct flow, Arnold-Chiari malformation or Dandy–Walker malformation.[5] these patients
may stabilize in later years due to compensatory mechanisms but may
decompensate, especially following minor head injuries. During these
decompensations, determining the extent to which any new neurological deficits
may be due to the new acute event, compared with hydrocephalus that may have
gone unnoticed for many years, is difficult.
Hydrocephalus Signs and Symptoms
Symptoms of hydrocephalus are determined by the following factors:- Age
- Degree of ventricular enlargement
- Rate of hydrocephalus development
- Type
- Underlying condition
Symptoms of Hydrocephalus in Infants
The characteristic symptom seen in infants is enlargement of the head. An infant's skull expands to accommodate excess CSF because the bones of the skull have not closed yet.Very young children commonly experience irritability, poor feeding, and lethargy.
Symptoms of Hydrocephalus in Children and Adults
Children and adults may experience the following symptoms:- Blurred or double vision
- Cognitive difficulties
- Downward gaze or "sun-setting eyes"
- Headache
- Imbalance and dizziness
- Incontinence
- Irregular gait
- Lethargy
- Nausea
- Poor coordination
- Visual disturbances
- Vomiting
- Weakness
Diagnosis of Hydrocephalus
If you think that you or someone you care about may have hydrocephalus, we recommend you learn about the symptoms and diagnostic tests for this condition. We also encourage you to trust your instincts. If you notice changes or have an intuitive feeling that something is not right with the person you are concerned about, act on that feeling and seek medical attention.Only a medical doctor can make a diagnosis of hydrocephalus. The information here is intended to help you understand and navigate through the process of seeking medical advice. In children, it is often a pediatrician who first suspects hydrocephalus. A pediatric neurosurgeon will typically make the final diagnosis. In adults, hydrocephalus is often diagnosed by a neurologist working with a neurosurgeon.
If you have already received a diagnosis, the information below will help you make sense of the classifications and causes of hydrocephalus.
Symptoms and Diagnostic Tests
Symptoms of untreated hydrocephalus are variable. During pregnancy, routine ultrasound can detect enlarged ventricles (spaces) within the baby’s brain. In children the symptoms tend to be related to high pressure and may include nausea, vomiting, headache and vision problems. In young and middle aged adults symptoms run the gamut of those seen in children and in older adults and most often include dizziness and vision problems. In older adults with NPH the symptoms are more likely to be loss of function in three main areas: walking, thinking and bladder control.| Infants and Children | Young & Middle Aged Adults | Older Adults (NPH) |
| Abnormal Head Enlargement | Difficulty Walking | Difficulty Walking |
| Tense, Bulging Fontanel | Cognitive Challenges | Cognitive Challenges |
| Prominent Scalp Veins | Urinary Urgency or Incontinence | Urinary Urgency or Incontinence |
| Skull bones may feel seperated | Chronic Headaches | |
| Vomiting, Sleepiness, Irritability | ||
| Headache, Nausea, Vomiting, Vision | ||
| Downward Deviation of Eyes |
Acute hydrocephalus treatment
For initial treatment of acute hydrocephalus one will initially use
medicines which reduce CSF production, and lumbar punctures. Mesurements of
inter-cranial pressure, and the various scanning techniques are used to asses
the further treatment.
If the CSF pressure does not return to normal other methods may be
used to release the pressure such as "ventricular taps" where the CSF is drained
dirrectly from the ventricule.
After some time it will become clear wether the increase in
pressure has stopped, or has become continuous and requires surgical treatment.
Treating the causes
Treatment of the causative factors is the best strategy. When the
ventricles are enlarged one needs to determine the cause. In the case of
obstructive hydrocephalus, an unequal enlargement of the ventricles will point
to the location of the obstruction. Causative factors for the obstruction are
then searched for. Tumours or blood clots can obstruct the CSF pathways, and
their removal can often re-establish a normal CSF flow pathway. Obstruction at
the aqueduct or the outlets of the fourth ventricle can often be treated by
surgically creating a new outlet for the ventricles, through the floor of the
third ventricle (third ventriculostomy). Blockage of the foramen of Monroe with
a resultant trapped lateral ventricle can be treated by surgically creating a
window through the curtain of tissue separating the two lateral ventricles
(septal fenestration).
Endoscopy operations involve inserting a small endoscope into the
ventricle through a single small hole in the skull. The endoscope is connected
via a micro-camera to a television monitor on which the surgeon can see inside
the ventricles. Using these endoscopes, neurosurgeons can now create a bypass,
allowing CSF to flow around certain blockages and restoring normal flow. Only
certain patients are eligible for endoscopic surgery, and the patients must be
selected carefully. In particular, patients with blockages within the ventricles
themselves (those with obstructive hydrocephalus) are potentially candidates for
endoscopic surgery.
When the CT or MRI scans show a case of hydrocephalus which cannot
be dealt with using one of the above techniques, a permanent device needs to be
surgically implanted to draw the fluid out of the ventricles and to carry it to
some other cavity within the body where it will be reabsorbed into the blood
stream. Such devices are called shunts and they became practical in the 1950's
when common problems with hydrocephalus treatments were being solved. These
consisted of rejection of the tubing by the body's defences, as well as
infections and blockages of the tube.
ليست هناك تعليقات:
إرسال تعليق